

Abstract
Traditional cognitive theories often characterize Major Depressive Disorder (MDD) as a dysfunction of unnatural negative emotions and thoughts. This essay employs the Predictive Processing (PP) framework to identify the core issue of MDD as a state of distorted and rigid predictive inference. First, the excessively precise negative priors foster cognitive rigidity against belief updates regardless of the emotional valence of disconfirming evidence. Second, a passive, yielding error minimization strategy results in an attentional bias towards negative confirming information, alongside an “inactive” mode of active inference through disengagement from the environment. Finally, the concept of allostasis provides the neurobiological foundation to unite these mechanisms, with the aim of energy conservation when high learning costs for belief updates are required in chronic stressful environments. By reframing MDD as an inefficient yet strategic computational retreat, this new model will inspire novel psychiatric treatments to restore the expectational plasticity and contribute to the destigmatization of depression.
When Beliefs Stop Updating: A Predictive Processing Account of Major Depression
Depression is commonly defined and perceived by the public as a mood disorder. According to the American Psychiatric Association (2013), major depressive disorder (MDD) is characterized by symptoms of a persistent depressed mood (e.g., feelings of sadness, emptiness, and hopelessness) and a loss of interest or pleasure. Although the exact cause of MDD remains unknown, numerous biological, social, and psychological or personal factors have been identified as risk factors, and various theories have been proposed to explain the mechanism underlying depressive symptoms. The most prominent cognitive model regarding the belief systems of depressed individuals is Aaron Beck’s cognitive triad, which involves an automatic negative thinking loop consisting of the self, the world, and the future driven by negative self-schema (Beck et al., 2024). This theoretical focus on pessimistic explanatory styles accounting for MDD has been highly influential and fundamental to relevant investigations. Nevertheless, recent research has found evidence of bidirectional impacts between dysfunctional attitudes and distorted thoughts, with the distorted thoughts being more proximal and dysfunctional attitudes more distal to depressive symptoms (Pössel & Black, 2013). This suggests that distorted thoughts might play a more central role in the pathogenesis of MDD.
Predictive processing (PP) offers an evolutionary framework to explain the relationship between depression and cognitive distortion, aligning with empirical findings and incorporating a crucial active-perceptual dimension that traditional cognitive models overlooked. By applying PP to core depressive symptoms, this essay argues that MDD is not merely a mood disorder: It is more accurately a disorder of predictive inference in which the brain assigns excessively high precision to negative priors about the self and the world, thereby preventing belief updates in response to any kinds of disconfirming sensory evidence and inhibiting the active exploration of such evidence.
What is Predictive Processing
Predictive processing (PP) proposes that the brain is a “predictive engine” where top-down predictions of sensory inputs and bottom-up prediction errors (mismatched responses) together form a hierarchical, constantly updating model (Clark, 2013). This theory follows a Bayesian paradigm (Knill & Pouget, 2004): higher-level cortical areas of the brain generate a prior—a probability distribution of what is expected to happen. Incoming sensory signals in lower-level areas will be compared to prior expectations. When a mismatch occurs, it is registered as a prediction error, and it will provide feedback to update internal beliefs and form a posterior. Within this framework, the ultimate goal of human cognition is to minimize prediction errors.
Whether the brain actually updates its belief when facing a prediction error, however, depends on the precision (estimated reliability) of the prior and the precision weighting of sensory data. Precision weighting means assigning reliability to the signals; if the brain perceives the incoming signals as imprecise (i.e., “noisy”), then the prior will maintain its dominance and the internal beliefs will remain unchanged (Kanai et al., 2015).
Active inference is a second, complementary mechanism of PP for error minimization. While perceptual inference changes the internal model to fit the world, active inference involves taking actions to change the world in order to fulfill internal predictions. This concept resolves the “dark room” paradox: Agents do not stay in an environment deprived of sensory signals to avoid surprise because they possess priors for movements and explorations of their surroundings (Friston et al., 2012). I will now connect these core PP ideas to the understanding of depression.
Depression as Dysfunctional Precision Weighting
Major depressive disorder (MDD) can be conceptualized as a state of dysfunctional precision weighting. Individuals with MDD often hold highly precise negative priors across a wide range of domains, while positive, disconfirming sensory data are assigned low precision. In other words, depressed individuals would down-weight or “filter out” positive information that potentially could have changed their negative expectations. The psychological term cognitive immunization clearly portrays this procedure. Cognitive immunization is the reappraisal of expectation-disconfirming experiences to preserve existing beliefs (Rief et al., 2015). For example, a student receiving an unexpectedly high test score might conclude: “I was just too lucky this time. I’m actually not good at this subject and won’t achieve this again.” Experimental promotion of cognitive immunization strategies demonstrates a significant increase in the persistence of negative expectations (Kube et al., 2018), which implies that MDD patients may be constantly utilizing low-precision weighting techniques for positive information.
Kube et al. (2020) proposed an expectation-focused model for MDD based on the PP framework to describe these dynamics (Figure 1). Following this model, when a positive sensory signal contradicts a negative prior, healthy individuals update their expectation accordingly, while depressed individuals would use cognitive immunization to maintain their original negative beliefs. Conversely, when a negative signal contradicts a positive expectation, depressed individuals update their beliefs immediately, whereas healthy individuals would use cognitive immunization to sustain their original positive beliefs. This model is theoretically plausible but not perfectly in line with later empirical findings. Research indicates that depressed people do show a weaker increase in positive expectations following positive feedback compared to healthy people (Würtz et al., 2024). This suggests MDD is correlated to a lesser degree of positive belief updates, but not to a full extent of cognitive immunization, as depressed individuals do incorporate some positive signals to form a more positive posterior. Similarly, a meta-analysis has found a small yet significant association between depressive symptoms and deficits in positive belief updating (Zabag et al., 2025).
Figure 1
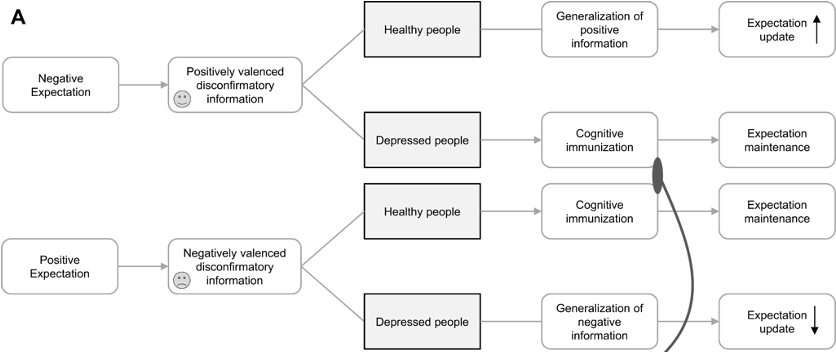
Expectation update vs. maintenance in healthy vs. depressed people
Note. Adapted from Distorted Cognitive Processes in Major Depression: A Predictive Processing Perspective by T. Kube et al., 2020, Biological psychiatry. Copyright 2020 by Elsevier.
However, when examining the interaction between positive expectations and negative signals, depressive symptoms are not found to be associated with an increased sensitivity to negative information, nor a greater integration of such signals (Kube & Glombiewski, 2021). Moreover, a reduced capacity for belief updating appears to occur in MDD regardless of the emotional valence of disconfirming sensory data (Liknaitzky et al., 2017). These updating deficits are more complicated than simple negative biases, because they also indicate that individuals with MDD do not necessarily shift toward negative beliefs quickly when a positive prior is confronted by negative disconfirming signals. Instead of a one-sided cognitive immunization against positive information, perhaps a “double-bind” rigidity better captures the essence of dysfunctional precision weighting in MDD. In this sense, the primary pathology is not the content of the belief, but the system’s inability to update itself in the face of any contradictory evidence.
Cognitive rigidity, or the lack of cognitive flexibility, refers to the difficulty of adapting to novel environments or switching between modes of thinking (Cools, 2019). Depressed individuals experience challenges in updating expectations across a variety of contexts. Even when they receive negative feedback contradicting their positive expectations, they still tend to stick to the established thinking patterns, updating their beliefs significantly more slowly than healthy individuals (Sacco & Hokanson, 1982). In addition, healthy individuals display an optimism bias by updating expectations more readily following positive signals than negative ones (Hobbs et al., 2022). This suggests that healthy cognition not only has lower levels of cognitive rigidity, but also assigns higher precision to positive disconfirming information.
Synthesizing these findings, a more robust PP-inspired model of expectations in MDD can be derived. Individuals with MDD hold excessively precise priors with overwhelmingly negative content. This creates a two-fold barrier to belief updating: On one hand, because their negative priors are so dominant, they rarely even predict positive outcomes, which reduces the overall chances of making belief updates for the prediction errors from negative disconfirming evidence. On the other hand, their precise priors lead to profound cognitive rigidity: They weigh external sensory data, irrespective of emotional valence, with low precision, thus preventing the standard Bayesian update when receiving disconfirming evidence. This explains why depressed patients frequently exhibit cognitive immunization against positive disconfirming signals, as these are just more common circumstances to be witnessed. The disparity between healthy and depressed states is further magnified by the asymmetric precision weighting found in healthy individuals, whose amplification of positive disconfirming evidence sharpens the contrasts with MDD’s negatively anchored reality.
Biased Attention and Constrained Active Inference of Depression
Recurrent uncontrollable negative thoughts, or rumination, are a hallmark of depressive symptoms (Nolen-Hoeksema et al., 2008). This section will address why depressed people tend to be “trapped” in a vicious cycle of negative thoughts, even though they are not more actively engaged in the search for prediction errors from negative evidence. In fact, they might be utilizing a passive prediction error minimization strategy distinct from that of healthy individuals.
To elaborate on the inquisition of the previously proposed MDD’s expectation model, the implication of attention within the PP framework should be introduced. Essentially, attention is the process of optimizing precision weights, where individuals predict what sensory signals will provide more reliable information to satisfy the goal of minimizing prediction error (Slagter & van Moorselaar, 2021). In this sense, signals that are given more attention are expected to come up with more prediction errors, so that the brain can adjust beliefs promptly. Most research agrees that MDD involves a negative attentional bias: Depressed individuals focus disproportionately on negative stimuli (Dainer-Best et al., 2017) and are more engaged in the internal processing of negative information (Santesso et al., 2008). A negative self-reinforcement loop, or vicious cycle, is used to describe how depressed people’s biased attention leads to increased negative affect, strengthening dysfunctional behaviors, and further reinforcing the attentional bias (Wittenborn et al., 2015). If attention is equivalent to precision weighting, then negative stimuli are assigned with higher precision by MDD patients. According to PP, these individuals are actually looking for negative disconfirming data to be an error for their positive priors, thus forming negative posteriors. This is at odds with the claim that all kinds of belief updates are not welcomed in the MDD cognitive system.
Yet another angle can be taken on why depressed people display a negative attentional focus. It is not an active search for prediction errors, but rather a static, compliant prediction error minimizing process. Usually, healthy people would use active inference to manipulate their environment to match their priors. For instance, if a student holds a prior expectation of being high-achieving, they will study hard and attend office hours so that the resulting test grades will be high and align with their expectation. Depressed people, on the contrary, do not utilize active inference as frequently. Or, to put it another way, their inferences are fulfilled more through inaction, the lack of behavioral manipulations of the external environment. An easier method to minimize prediction errors is not to take physical actions, but to pay more attention to signals that will not cause surprise, i.e., focusing on negative data that align with their substantially negative priors. A student with a rigid prior of “I am a failure” will give up the effort of studying hard; without participation in activities that could change the external sensory signals (the grades), they will not encounter prediction errors when seeing a naturally low-grade result. Consequently, depressed people cling to negative stimuli in order not to actively trigger belief updates, which in turn creates a deceptive illusion of the prediction error being minimized. Using the “dark room” analogy, MDD patients are those who stagnate in the dark room to avoid any kind of surprise. In short, MDD manifests a tendency to rest in negative confirming signals because the prediction errors are unlikely to emerge from within.
Relevant psychology research has pointed out the nuances of MDD’s attentional mechanism. Depressed individuals may not automatically orient their attention toward negative information, but once such information has come to be the focus, they have greater difficulty disengaging from it (Gotlib & Joormann, 2010). Studies using eye-tracking technology indeed find no group difference in initial attention orientation (Suslow et al., 2020); once dysphoric images and sad faces come into attention, depressed participants find it more difficult to disengage their gazes (Sanchez et al., 2013), supporting a late-stage attentional maintenance. Negative signals, therefore, are not assigned with higher precision weights pre-attentively, but are instead maintained in cognition for a longer time. Besides, rumination, in addition to being a maladaptive emotion regulation strategy, can be seen as a prolonged attentional control to prevent the search for disconfirming evidence and prediction errors. High ruminators have shown impaired attentional switching in working memory, with the strongest impairment occurring when the information switches away from negativity (Koster et al., 2013). A neurophysiological study has also detected more neural resources being required to switch between affective items when ruminators were in a sad mood (Chuen Yee Lo et al., 2012).
While a quantitative measure for active inference has not been established in empirical studies, several strands of data suggest that people with more severe depressive symptoms are less likely to take behavioral actions in general, alluding to non-exploratory active inference strategies. A systematic review has found that depressed people show reduced willingness to expend cognitive and especially physical effort for rewards (Horne et al., 2021). Behavioral avoidance is another facet of inaction, and individuals with depression report higher levels of behavioral avoidance across social and nonsocial domains (Takagaki & Yokoyama, 2024). The negative self-reinforcement loop of MDD actually corresponds well to the idea of constrained active inference, since it contains behavioral avoidance, withdrawal, or isolation at its core. The negative schema, affect, and perceived stress in this loop all eventually manifest in inaction. In the long run, depressed people tend to miss out on pleasurable activities due to their physical bodily lethargy— they just do not externally act in ways that might cause prediction errors.
Putting all the pieces together, I will give a brief summary of the comprehensive theoretical framework I have proposed for MDD’s mechanisms with reference to PP: In order to minimize prediction errors, depressed people engage in passive, locked-in computational predictive inferences with the intention of not actively causing belief updates. Their brains form extensive, rigid negative priors and treat all external sensory signals as imprecise, so that disconfirming evidence is less likely to be captured. They also avoid exploratory active inferences, so that the natural negative outcomes of inaction fulfill their negative priors.
Allostatic Inefficiency: Neurobiological Root of Depression
Barrett et al.(2016) proposed a predictive mind theory focusing on interoception and allostasis, revealing how they characterize MDD. This neurobiological framework provides an important account for unifying the cognitive deficits of MDD through the lens of an overall reduced metabolic energy for both perception and action.
Allostasis is the process through which the human brain maintains energy regulation by anticipating the body’s needs (e.g., glucose, water, oxygen, electrolytes, etc.) and preparing to satisfy those needs before they arise (Sterling, 2012). Linking allostasis to PP, the brain constantly predicts what the body requires to survive based on interoception, the perception of internal bodily signals and bodily states (Schmitt & Schoen, 2022). This reflects an active inference process. Accordingly, prediction error represents not only a computational mismatch, but also an energy expenditure. When a prediction error occurs in perception, physiological arousal is triggered (Barrett & Campbell, 2017) as the brain attempts to learn and integrate the new information through neural activities like modification of synaptic connections (Ramirez & Arbuckle, 2016). For healthy people, energy input and expenditure are typically well-balanced. However, if the energy demands exceed supply, then an allostatic overload would force the system to restore the energy balance by reducing metabolic cost (McEwen & Wingfield, 2003) — namely, the prediction errors — for survival.
Therefore, MDD can be understood as an inefficiency of energy regulation over a relatively prolonged period of time, as past investments of metabolic energy largely disrupted the allostatic balance (Barett et al., 2016). This explains why chronic stress significantly increases the risk of developing depression (Hassamal, 2023): Stress induces a higher heart rate, greater prefrontal activation, and altered pupil dynamics, indicating that performance is maintained at a higher psychophysiological cost (Bobba-Alves et al., 2023). Other risk factors of MDD suggest similar high allostatic demands since more prediction errors need to be dealt with in volatile or punishing environments, such as aversive childhoods (McLaughlin et al., 2014), loss of social connections (Eisenberger, 2012), and poverty (Knifton & Inglis, 2020). To resolve the allostatic overload, depressed individuals have to decrease their energy expenses. In terms of perception, they reduce the precision weights assigned to the external information to avoid the energy-intensive learning processes. In terms of action, they minimize the expected energy consumption of future bodily states, resulting in psychomotor retardation.
In particular, this energy regulation strategy is inefficient because dominant negative priors would predict higher energy costs for a belief-updating process than those costs actually are. Dysregulated allostasis is then perceived as harder to resolve, leading to a reduced likelihood of searching for prediction errors and updating expectations for bodily needs. Due to the exaggerated perceived costs of any active behavior, MDD patients might, in the end, never be able to restore the allostatic balance without psychiatric treatment.
Concluding Remarks
In conclusion, this essay describes the phenomenological mechanisms of major depressive disorder (MDD) as a dysfunction of the brain’s predictive machinery in maintaining a flexible and sustainable model of self and the world. Cognitive rigidity against disconfirming sensory data and the attentional bias toward negative, confirming sensory data exemplify a passive prediction error minimization strategy, with a neurobiological basis in inefficient energy regulation stemming from allostatic overload.
Historically, depression has often been conceptualized as an unnatural cognitive breakdown, defined by “partially insane” moods and illogical thought patterns (Kendler, 2020). However, from the viewpoint of Predictive Processing (PP), MDD is increasingly characterized as a rational defensive system, where the Bayesian brain determines that the best strategy in response to stressful environments is to enter a computational “safe mode”. By assigning excessively precise negative priors, the agent successfully minimizes unexpected uncertainty and conserves metabolic energy. Although this regulation is ultimately inefficient and will severely impair daily functioning, an adaptive narrative will hopefully mitigate the stigma against depressed individuals and promote a more empathetic understanding of the struggles they experience.
Furthermore, this novel, unified PP theory of MDD sheds new light on the understanding of many effective depression treatments, including psychotherapy and pharmacology. For example, Cognitive Behavioral Therapy (CBT) aims at lowering the precision of rigid negative priors, Behavioral Activation (BA) incentivizes active inferences to break the cycle of withdrawal, while pharmacological interventions chemically create a physiological window of plasticity. This deeper understanding also paves the way for new cognitive therapies to target the mechanics of dysfunctional predictive inference directly. Future research can conduct more thorough investigations in this vein, moving beyond the content of depressive thoughts and into the retraining of the brain’s ability to trust, sample, and learn from its environment once again.
References
American Psychiatric Association. (2013). Depressive disorders. In Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596.dsm05
Barrett, L. F., & Campbell, C. (2017). How emotions are made: The secret life of the brain. Brilliance Audio.
Barrett, L. F., Quigley, K. S., & Hamilton, P. (2016). An active inference theory of allostasis and interoception in Depression. Philosophical Transactions of the Royal Society B: Biological Sciences, 371(1708), 20160011. https://doi.org/10.1098/rstb.2016.0011
Beck, A. T., Rush, A. J., Shaw, B. F., Emery, G., DeRubeis, R. J., Hollon, S. D., & Clark, D. M. (2024). Cognitive therapy of depression. Guilford Publications.
Bobba-Alves, N., Sturm, G., Lin, J., Ware, S. A., Karan, K. R., Monzel, A. S., Bris, C., Procaccio, V., Lenaers, G., Higgins-Chen, A., Levine, M., Horvath, S., Santhanam, B. S., Kaufman, B. A., Hirano, M., Epel, E., & Picard, M. (2023). Cellular allostatic load is linked to increased energy expenditure and accelerated biological aging. Psychoneuroendocrinology, 155, 106322. https://doi.org/10.1016/j.psyneuen.2023.106322
Chuen Yee Lo, B., Lau, S., Cheung, S., & Allen, N. B. (2012). The impact of rumination on internal attention switching. Cognition & Emotion, 26(2), 209–223. https://doi.org/10.1080/02699931.2011.574997
Clark, A. (2013). Whatever next? Predictive brains, situated agents, and the future of cognitive science. Behavioral and Brain Sciences, 36(3), 181–204. doi:10.1017/S0140525X12000477
Cools, R. (2019). Chemistry of the adaptive mind: Lessons from dopamine. Neuron, 104(1), 113–131. https://doi.org/10.1016/j.neuron.2019.09.035
Dainer-Best, J., Trujillo, L. T., Schnyer, D. M., & Beevers, C. G. (2017). Sustained engagement of attention is associated with increased negative self-referent processing in major depressive disorder. Biological Psychology, 129, 231–241. https://doi.org/10.1016/j.biopsycho.2017.09.005
Eisenberger, N. I. (2012). The pain of social disconnection: Examining the shared neural underpinnings of physical and social pain. Nature Reviews Neuroscience, 13(6), 421–434. https://doi.org/10.1038/nrn3231
Friston, K., Thornton, C., & Clark, A. (2012). Free-energy minimization and the dark-room problem. Frontiers in Psychology, 3. https://doi.org/10.3389/fpsyg.2012.00130
Gotlib, I. H., & Joormann, J. (2010). Cognition and depression: Current status and Future Directions. Annual Review of Clinical Psychology, 6(1), 285–312. https://doi.org/10.1146/annurev.clinpsy.121208.131305
Hassamal, S. (2023). Chronic stress, neuroinflammation, and depression: An overview of pathophysiological mechanisms and emerging anti-inflammatories. Frontiers in Psychiatry, 14. https://doi.org/10.3389/fpsyt.2023.1130989
Hobbs, C., Vozarova, P., Sabharwal, A., Shah, P., & Button, K. (2022). Is depression associated with reduced optimistic belief updating? Royal Society Open Science, 9(2). https://doi.org/10.1098/rsos.190814
Horne, S. J., Topp, T. E., & Quigley, L. (2021). Depression and the willingness to expend cognitive and physical effort for rewards: A systematic review. Clinical Psychology Review, 88, 102065. https://doi.org/10.1016/j.cpr.2021.102065
Kanai, R., Komura, Y., Shipp, S., & Friston, K. (2015). Cerebral hierarchies: Predictive Processing, precision and the Pulvinar. Philosophical Transactions of the Royal Society B: Biological Sciences, 370(1668), 20140169. https://doi.org/10.1098/rstb.2014.0169
Kendler, K. S. (2020). The origin of our modern concept of depression—the history of melancholia from 1780-1880. JAMA Psychiatry, 77(8), 863. https://doi.org/10.1001/jamapsychiatry.2019.4709
Knifton, L., & Inglis, G. (2020). Poverty and mental health: Policy, practice and research implications. BJPsych Bulletin, 44(5), 193–196. https://doi.org/10.1192/bjb.2020.78
Knill, D. C., & Pouget, A. (2004). The Bayesian Brain: The Role of uncertainty in neural coding and computation. Trends in Neurosciences, 27(12), 712–719. https://doi.org/10.1016/j.tins.2004.10.007
Koster, E. H. W., De Lissnyder, E., & De Raedt, R. (2013). Rumination is characterized by valence-specific impairments in switching of attention. Acta Psychologica, 144(3), 563–570. https://doi.org/10.1016/j.actpsy.2013.09.008
Kube, T., & Glombiewski, J. A. (2021). No evidence for the involvement of cognitive immunisation in updating beliefs about the self in three non-clinical samples. Cognitive Therapy and Research, 46(1), 43–61. https://doi.org/10.1007/s10608-021-10256-y
Kube, T., Rief, W., Gollwitzer, M., Gärtner, T., & Glombiewski, J. A. (2018). Why dysfunctional expectations in depression persist – results from two experimental studies investigating cognitive immunization. Psychological Medicine, 49(09), 1532–1544. https://doi.org/10.1017/s0033291718002106
Kube, T., Schwarting, R., Rozenkrantz, L., Glombiewski, J. A., & Rief, W. (2020). Distorted cognitive processes in major depression: A predictive processing perspective. Biological Psychiatry, 87(5), 388–398. https://doi.org/10.1016/j.biopsych.2019.07.017
Liknaitzky, P., Smillie, L. D., & Allen, N. B. (2017). Out-of-the-blue: Depressive symptoms are associated with deficits in processing inferential expectancy-violations using a novel cognitive rigidity task. Cognitive Therapy and Research, 41(5), 757–776. https://doi.org/10.1007/s10608-017-9853-x
McEwen, B. S., & Wingfield, J. C. (2003). The concept of allostasis in biology and Biomedicine. Hormones and Behavior, 43(1), 2–15. https://doi.org/10.1016/s0018-506x(02)00024-7
McLaughlin, K. A., Sheridan, M. A., & Lambert, H. K. (2014). Childhood adversity and neural development: Deprivation and threat as distinct dimensions of early experience. Neuroscience & Biobehavioral Reviews, 47, 578–591. https://doi.org/10.1016/j.neubiorev.2014.10.012
Nolen-Hoeksema, S., Wisco, B. E., & Lyubomirsky, S. (2008). Rethinking rumination. Perspectives on Psychological Science, 3(5), 400–424. https://doi.org/10.1111/j.1745-6924.2008.00088.x
Pössel, P., & Black, S. W. (2013). Testing three different sequential mediational interpretations of Beck’s cognitive model of the development of depression. Journal of Clinical Psychology, 70(1), 72–94. https://doi.org/10.1002/jclp.22001
Ramirez, A., & Arbuckle, M. R. (2016). Synaptic plasticity: The role of learning and unlearning in addiction and beyond. Biological Psychiatry, 80(9). https://doi.org/10.1016/j.biopsych.2016.09.002
Rief, W., Glombiewski, J. A., Gollwitzer, M., Schubö, A., Schwarting, R., & Thorwart, A. (2015). Expectancies as core features of Mental Disorders. Current Opinion in Psychiatry, 28(5), 378–385. https://doi.org/10.1097/yco.0000000000000184
Sacco, W. P., & Hokanson, J. E. (1982). Depression and self-reinforcement in a public and private setting. Journal of Personality and Social Psychology, 42(2), 377–385. https://doi.org/10.1037//0022-3514.42.2.377
Sanchez, A., Vazquez, C., Marker, C., LeMoult, J., & Joormann, J. (2013). Attentional disengagement predicts stress recovery in depression: An eye-tracking study. Journal of Abnormal Psychology, 122(2), 303–313. https://doi.org/10.1037/a0031529
Santesso, D. L., Steele, K. T., Bogdan, R., Holmes, A. J., Deveney, C. M., Meites, T. M., & Pizzagalli, D. A. (2008). Enhanced negative feedback responses in remitted depression. NeuroReport, 19(10), 1045–1048. https://doi.org/10.1097/wnr.0b013e3283036e73
Schmitt, C. M., & Schoen, S. (2022). Interoception: A multi-sensory foundation of participation in Daily Life. Frontiers in Neuroscience, 16. https://doi.org/10.3389/fnins.2022.875200
Slagter, H. A., & van Moorselaar, D. (2021). Attention and distraction in the predictive brain. Visual Cognition, 29(9), 631–636. https://doi.org/10.1080/13506285.2021.1936733
Sterling, P. (2012). Allostasis: A model of predictive regulation. Physiology & Behavior, 106(1), 5–15. https://doi.org/10.1016/j.physbeh.2011.06.004
Suslow, T., Hußlack, A., Kersting, A., & Bodenschatz, C. M. (2020). Attentional biases to emotional information in clinical depression: A systematic and meta-analytic review of Eye Tracking Findings. Journal of Affective Disorders, 274, 632–642. https://doi.org/10.1016/j.jad.2020.05.140
Takagaki, K., & Yokoyama, S. (2024). Association between the behavioral activation mechanism and depression severity: Focusing on avoidance patterns of university students. Behavioral Sciences, 14(8), 713. https://doi.org/10.3390/bs14080713
Wittenborn, A. K., Rahmandad, H., Rick, J., & Hosseinichimeh, N. (2015). Depression as a systemic syndrome: Mapping the feedback loops of major depressive disorder. Psychological Medicine, 46(3), 551–562. https://doi.org/10.1017/s0033291715002044
Würtz, F., Kube, T., Woud, M. L., Margraf, J., & Blackwell, S. E. (2024). Reduced belief updating in the context of depressive symptoms: An investigation of the associations with interpretation biases and self-evaluation. Cognitive Therapy and Research, 48(2), 225–241. https://doi.org/10.1007/s10608-023-10454-w
Zabag, R., Vander Zwalmen, Y., Kube, T., Hoorelbeke, K., Koster, E. H. W., & Joormann, J. (2025). Belief updating deficits in depression: A systematic review and meta-analysis. Clinical Psychology Review, 121, 102649. https://doi.org/10.1016/j.cpr.2025.102649

Leave a comment